{kind=link}
By Christine H. Monahan, Karen Davenport, Julia Burleson, and Kennah Watts
The price patients pay for outpatient services often depends on where they receive care. Throughout the country, consumers, employers, and insurers typically pay significantly higher prices for care at hospital outpatient departments (HOPDs) than the same care at independent physician offices or ambulatory surgical centers (ASCs). As hospitals continue to acquire independent practices, more care is shifting into these high-cost settings, driving up premiums and out-of-pocket costs for millions of Americans.
In response, Congress and federal officials have taken steps to begin eliminating site-of-service differences in Medicare by establishing the same payment rate for the same service regardless of whether it is provided in a hospital-owned facility or an independent setting. Policymakers at the state and federal levels have begun eyeing similar site-neutral payment reform options for the commercial health insurance market, where site-of-service differences can be particularly wide.
In our new resource, Site-Neutral Payment Reform and the Commercial Market, we explore drivers behind the need for reform and outline the rationale for adopting a site-neutral approach. We then present a comprehensive framework for designing site-neutral payment policies in the commercial health insurance market, highlighting a range of options and key considerations across four core decision domains.
Why Reform Is Urgent: The HOPD Payment Premium
Facility fees for outpatient services in HOPDs, along with the increased market power hospitals often gain through consolidation, drive higher payments for services delivered in these settings compared to physician offices and ASCs.
- Split Billing and Site-of-Service Differences: HOPDs and the clinicians working there typically issue two separate bills for a single service: a professional fee for the clinician’s labor and a facility fee intended to cover hospital overhead. In contrast, a physician office charges a single fee that covers both labor and overhead. The total payment for outpatient care in HOPDs—which includes both facility and professional fees—is generally much higher than the payment an independent physician office receives. For routine outpatient services such as clinic visits, diagnostic testing, and drug administration, payment for care at an HOPD may be three times as much as a physician office.
- Provider Consolidation: Hospitals and health systems have steadily acquired physician practices, turning physician offices and ASCs into higher-priced HOPDs. This vertical integration between hospitals and other types of providers also gives health systems greater leverage in contract negotiations with payers and increases prices. The potential for higher rates creates further incentive for consolidation and integration in a self-reinforcing cycle.
Hospitals often justify these higher charges by citing higher costs associated with specialized care requirements, emergency standby capacity, or more complex patient populations. However, research suggests these explanations are often incomplete. For instance, the Medicare Payment Advisory Commission (MedPAC) found only small differences in patient severity between hospital and freestanding settings for the types of services that might be paid on a site-neutral basis, and that these differences had no significant effect on hospital charges. Furthermore, hospitals can continue to address any distinctions in patient severity by billing those more complex patients at a higher service level or for the additional services they require, rather than maintaining inflated payments across the board.
Learning from Medicare
Medicare’s efforts inform a growing interest in adopting site-neutral reforms to the commercial market. Among major health insurance programs, only Medicare requires site-neutral payments, and only in limited circumstances. Explore our resource “What You Need to Know About Medicare Site-Neutral Payment Reform” for more information.
The Economic Case for Site-Neutrality
The financial impact of site-neutral payment reform could be significant for both state and national budgets:
- National Savings: Nationwide implementation of site-neutral payment in the commercial market for MedPAC-identified services could save $58 billion in a single year (based on 2022 data). Over a decade, these savings could total $898 billion, potentially reducing employer-sponsored insurance premiums by 5 percent.
- State-Level Savings: New York’s Fair Pricing Act proposal to cap commercial payments at 150 percent of Medicare rates for MedPAC-identified services in on- and off-campus HOPDs could yield $1.1 billion in annual statewide savings.
- Consumer Protection: Site-of service differences drive higher health insurance premiums and can also increase cost-sharing for consumers who receive care at HOPDs. The Committee for a Responsible Federal Budget estimates that its three-part site-neutrality proposal would lower premiums by $386 billion over ten years while reducing consumers’ cost-sharing responsibilities by $73 billion over the same timeframe. Consumer out-of-pocket savings under the New York Fair Pricing Act are estimated to range between $168.9 million to $213.4 million per year in 2022 dollars.
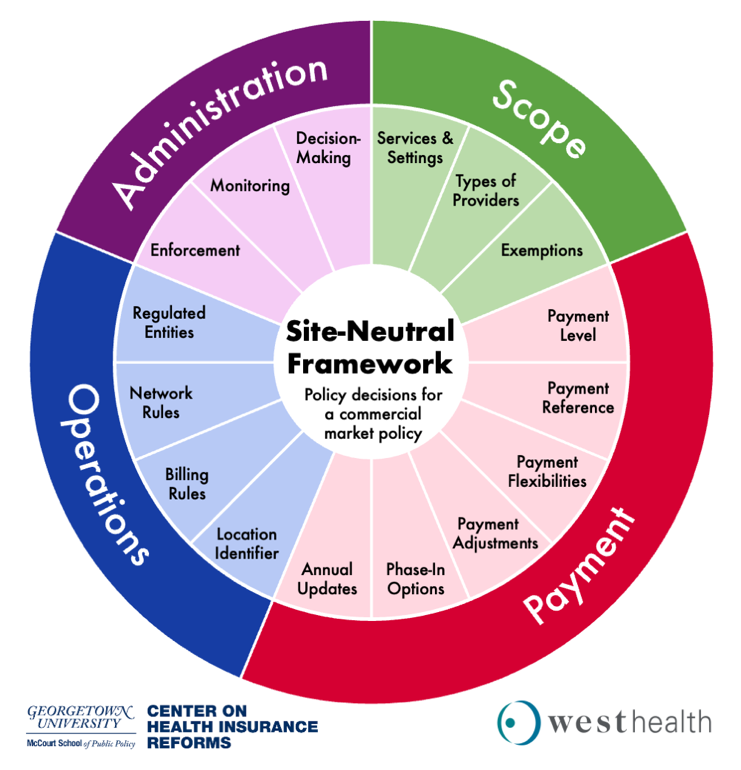
The Four Decision Domains for a Site-Neutral Policy
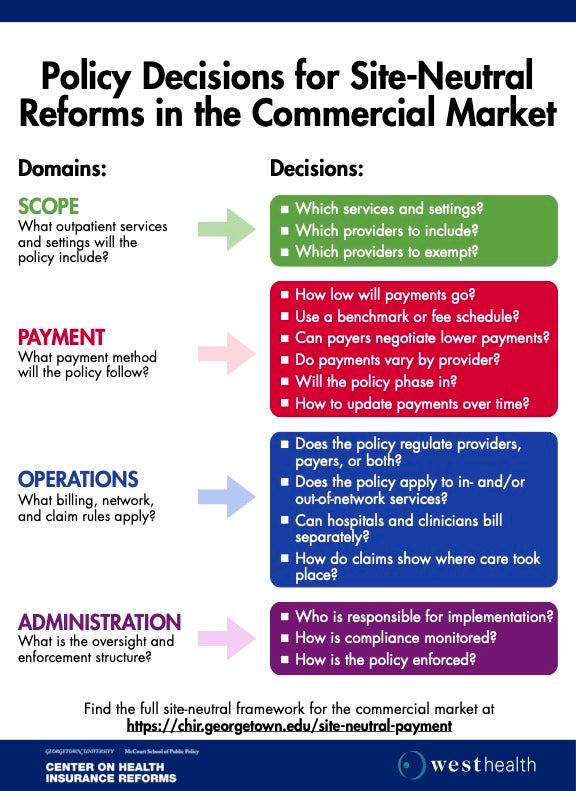
Crafting an effective site-neutral policy requires navigating complex operational and administrative questions. Policymakers must address four central domains:
- Scope: Policymakers must decide which services, settings, and providers are regulated. A broad approach might include all services that are safe for delivery at a physician office or ASC. They must also consider whether to exempt specific facilities, such as dedicated emergency departments, or make adjustments or phase-in requirements for certain types of hospitals that may be financially vulnerable.
- Payment Methodology: To ensure that a commercial site-neutral payment policy generates savings, policymakers need to create a payment methodology that puts specific bounds on what hospitals (and potentially other providers) can charge and updates these limitations over time.
- Operations and Billing: Implementation requires clear rules on who is regulated and how providers bill. For example, a commercial site-neutral payment policy could regulate the amount health care providers can charge and how they bill those charges, the amounts commercial payers reimburse for care, or both. Additionally, policymakers will need to set network and billing rules and may want to specify how providers identify the location of care on claims.
- Administration and Enforcement: Policymakers must determine the extent to which they define a commercial site-neutral payment policy’s scope of services, settings, and payment method in statute, versus delegating some or all of these decisions to regulatory bodies. They must also consider how to monitor and enforce a commercial-site neutral policy.
By thoughtfully addressing these domains, policymakers can help create a more affordable health care market that pays for care based the services provided—regardless of the site of care—and reduces payment incentives that encourage vertical integration and market consolidation.
Below, we include a one-pager of the various design questions for policymakers to consider: