

{kind=link}

Sabrina Corlette, Abigail Knapp, Stacey Pogue
The U.S. is in a health care affordability crisis, with consumers struggling to pay for health insurance and employers struggling to provide it. Texas is no exception, as the state faces rising health care prices that are reducing access to care and suppressing wage growth. As in many other states, Texas has experienced a high rate of health system consolidation, with monopolistic health systems leveraging their market power to bind employers and health insurers to profit-maximizing contracts. This increasing market dysfunction prompted Texas lawmakers in 2023 to enact legislation to blunt the anti-competitive effects of hospital monopolies, primarily by prohibiting certain clauses in provider-insurer contracts. Just over two years later, however, it is challenging to fully assess the impact of these reforms, in part because of loopholes that allow hospitals to continue to demand excessive prices.*
Background
The rise in consolidated hospital systems has driven up health care prices because these entities use their increased market power to extract higher reimbursement. In their negotiations with commercial insurers, many health systems require certain contracting clauses that constrain insurers from pursuing cost containment strategies that would empower employers and consumers to use lower-priced, higher-quality providers. These clauses include, for example:
- All-or-nothing: These clauses require insurers to contract with either all facilities and clinicians within a health system or none of them, regardless of an individual clinician or facility’s price or quality. In a highly consolidated market, this enables a dominant health system to raise prices for less-sought-after providers within the system.
- Anti-tiering. These clauses prevent insurers from sorting providers into different cost-sharing tiers based on price and quality of care, by requiring them to place the provider in the lowest cost-sharing tier, even if it does not meet the insurer’s standards for price and quality.
- Anti-steering: These clauses prohibit insurers from using cost-sharing or other incentives to steer patients to competing providers, even if those providers are less expensive or higher quality.
- Most-favored nation: These clauses prohibit providers from offering any other payer a lower price, preventing competing payers in the market from negotiating a lower cost contract with those providers.
- “Gag” clauses: These clauses prohibit contracting parties from disclosing information, such as the negotiated reimbursement rates, to outside entities, including to the employers or consumers who are ultimately paying for the coverage. Gag clauses in provider-payer contracts were prohibited under the Consolidated Appropriations Act of 2021. However, compliance has varied.
In a market with just one or two dominant health systems, insurers and employer health plans do not have the leverage to push back against cost-increasing contractual clauses. The same is true for providers in a market with just one or two dominant insurers.
Some states have attempted to curtail anti-competitive contracting through anti-trust oversight, but this can be resource-intensive (often requiring litigation). It is also narrow in impact, because any remedy, such as a requirement to remove an anti-competitive clause, would be limited to the parties involved in the contract.
The Texas Market
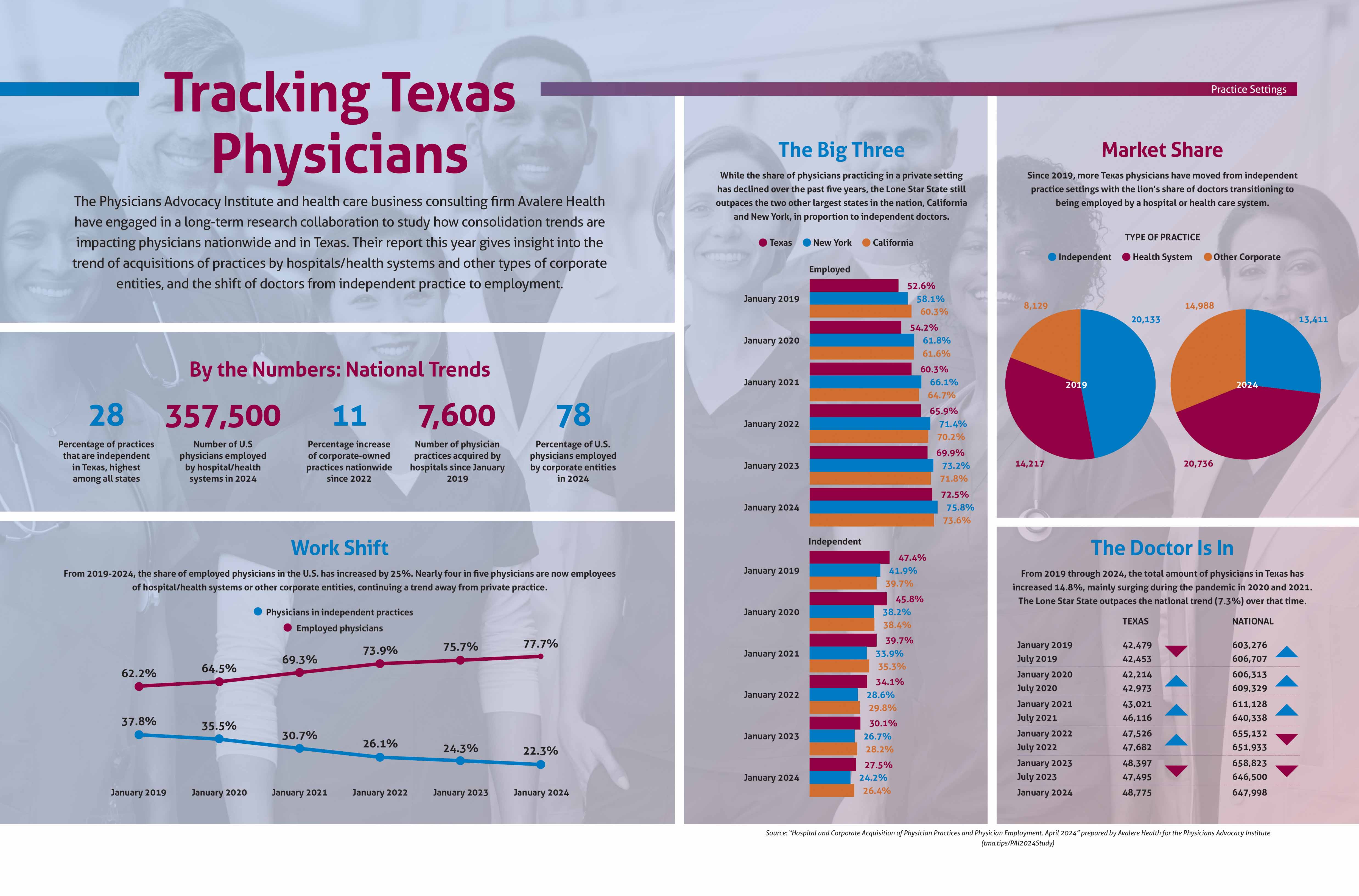
Consumers in Texas are bearing the brunt of an increasingly consolidated hospital market that is driving up employer and insurers’ costs and ultimately premiums. On average, employer health plans in Texas pay local hospitals over two-and-a-half times the Medicare reimbursement rate, but several hospitals are collecting between 290% and 320% of Medicare rates. In nine metropolitan areas, just one or two health systems control 100% of the market. As of 2020, over 60% of Texans lived in “highly” or “very highly concentrated” hospital metro areas, up from 36% in 2016. And 78% of Texas physicians are employed by hospitals, health systems, or other corporate entities. The result? Premiums for employer-sponsored insurance are rising faster than the rate of inflation and in 2023 averaged over $8000 per year for an individual, and almost $24,000 per year for family coverage. In a recent Gallup poll, Texas ranked 50th in the country on health care costs due to the high burdens reported by its residents.,
{kind=link}
In Texas–A Market-Based Approach to Consolidation
It may surprise some that Texas is at the leading edge of states that have attempted to curtail onerous contracting clauses. A majority of the state’s lawmakers would likely say they are strong believers in the free market and oppose many forms of government regulation. But the legislative activity in Texas reflects a growing view that, in many parts of the state, the health care markets have become anything but free.
Leading up to the 2023 legislative session, lawmakers had become increasingly aware of the wide variance in prices that commercial insurers were paying for the same health care services, with the price largely dictated by the provider’s market power and not clinical quality or outcomes. In a functioning market, employers and insurers could design networks that prioritize efficient, high quality providers, and patients could make informed choices to reduce their out-of-pocket costs by using providers recognized for delivering value. But those kinds of choices were largely unavailable, due to anti-competitive contracts.
This market dysfunction prompted the Texas legislature to enact, in 2023, House Bill 711. The law bans four of the five anti-competitive contracting clauses listed above. Specifically, the bill disallows providers from entering into or renewing a contract that includes an anti-steering, anti-tiering, gag, or most favored nation clause. However, the law does not prohibit the “all-or-nothing” clause, in which dominant health systems require insurers to include all facilities and clinicians within the system in its network, or none of them. Although prohibiting such clauses was initially recommended by bill sponsors, physician lobbyists, including key physician-legislators, opposed the provision, arguing, somewhat hyperbolically, that it would “be an existential threat to hospitals, physician practices, and other medical providers and would allow health plans to choose who is put out of business and who wins in the healthcare ‘market.’”
Is the law working as intended?
Two years after enactment of HB 711, there’s little evidence that the rate of growth in health care prices has declined in Texas. Payers and advocates report that some dominant hospital systems continue to require all-or-nothing clauses in their contracts, a legislative loophole that has restricted plans’ ability to design networks that optimize efficiency and value. Further, in a few markets around the state, there is only one monopoly health system, limiting the pool of competing providers around which insurers could design networks and steer consumers via cost-sharing.
Looking Ahead
Texas advocates who supported the 2023 legislation are considering strategies for the next legislative session** that would enable closing the “all-or-nothing” loophole, so that employers and insurers would have more flexibility to decide which facilities and clinicians within a health system to contract with. However, lawmakers may also need to consider the reality that, in Texas’ most highly consolidated markets, simply taking away some anti-competitive contracting clauses will not be sufficient to curtail price gouging by monopolistic providers. In those parts of the state, more aggressive regulatory action may be needed.
*The authors greatly appreciate the willingness of several Texas health care stakeholders and advocates to share their views on the development and impact of HB 711. Their insights helped shape the drafting of this article.
**Texas’ legislature operates biennially, and will next meet in January 2027.